A distal femoral osteotomy requires an operation. The realignment necessary is determined during a scheduled consultation based on x-rays of all the lower limbs (hip-knee-ankle x-ray or EOS scan).
Before the operation, a pre-anaesthesia consultation is conducted to check the patient is physically apt to undergo the operation and minimise the risk of postoperative complications.
The operation takes place in an operating theatre in compliance with strict standards of cleanliness and safety. The patient is placed supine on an operating table and a tourniquet is placed around the thigh. The operation lasts about 1 hour and can be carried out under general or spinal anaesthesia. The latter is a regional anaesthetic anaesthetising the lower part of the body (as with an epidural). The anaesthetist will decide on the most suitable anaesthetic together with the patient.
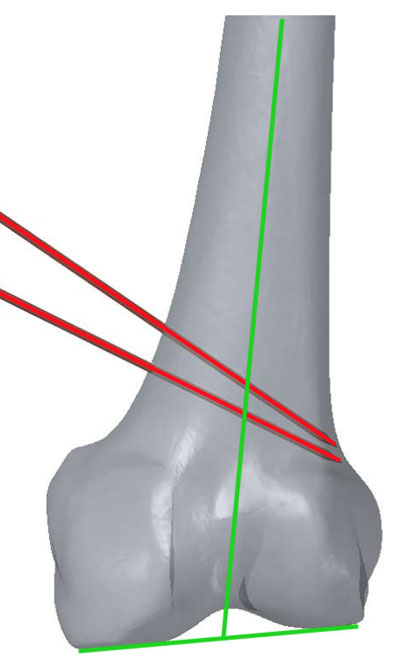
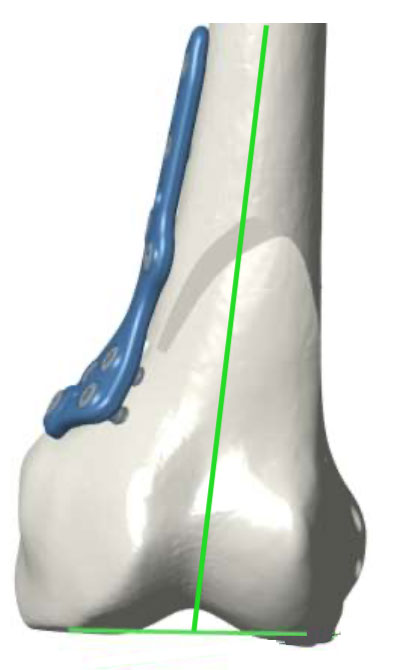
To perform a distal femoral osteotomy, an incision about 10 centimetres long on the lower, medial part of the thigh is necessary. Two cut lines are made in the femur and a wedge of bone is removed to realign the axis of the knee. The femur is then fixed with a plate.
A drain is inserted in the incision to prevent the formation of a haematoma.
After the operation, the knee is partially numbed with a nerve block to help improve postoperative pain management.
The effect lasts approximately 18 hours after the operation and can be prolonged with the insertion of a catheter in the thigh if the anaesthetist considers it necessary. Medication and ice on the knee also provide effective postoperative pain management.
After the operation, weight-bearing is not allowed on the leg operated on for 6 weeks and crutches must be used for walking.
Weight-bearing can then be resumed gradually. During this period, the knee can be mobilised during rehabilitation sessions. The knee may be immobilised in a brace while the bone heals.
The stay in hospital is often between 2 and 5 days.
The bone takes 2 to 3 months to heal, sometimes longer.
Several appointments are necessary to monitor the healing of the osteotomy.
The duration of medical leave depends on the patient’s occupation and is often between 2 and 4 months.
Driving can be resumed once weight-bearing is fully recovered. Sport can generally be resumed after 6 months.